Date
[Insert Claimant Name]
[Insert Claimant Address]
Dear [Insert Claimant Name]:
As a beneficiary under the Energy Employees Occupational Illness Compensation Program Act (EEOICPA), you are entitled to medical benefits for treatment of your [FAB: Insert Medical Condition, (ICD-Code), and effective date]. Covered medical services are payable in accordance with the fee schedules and medical benefits policies established under the Division of Energy Employees Occupational Illness Compensation (DEEOIC). Your medical benefits coverage includes payment to medical providers for care of your accepted work-related illness, such as medical appointments, hospitalizations, home and residential health care services (see attached Notice Regarding Home and Residential Health Care), medical appliances, supplies, and prescription medications.
Within the next few weeks, you will be receiving additional information regarding your medical benefits coverage. This will include a medical benefits identification card, along with an informational brochure explaining when and how to use your identification card. You will need to show this card to your physician, or other enrolled medical provider, as it contains billing instructions explaining how physicians, hospitals, durable medical equipment suppliers, or other health care providers, can bill DEEOIC directly, so that you will not have to pay for medical treatment out-of-pocket. There are no deductibles for services or equipment as long as a DEEOIC enrolled medical provider bills for the services.
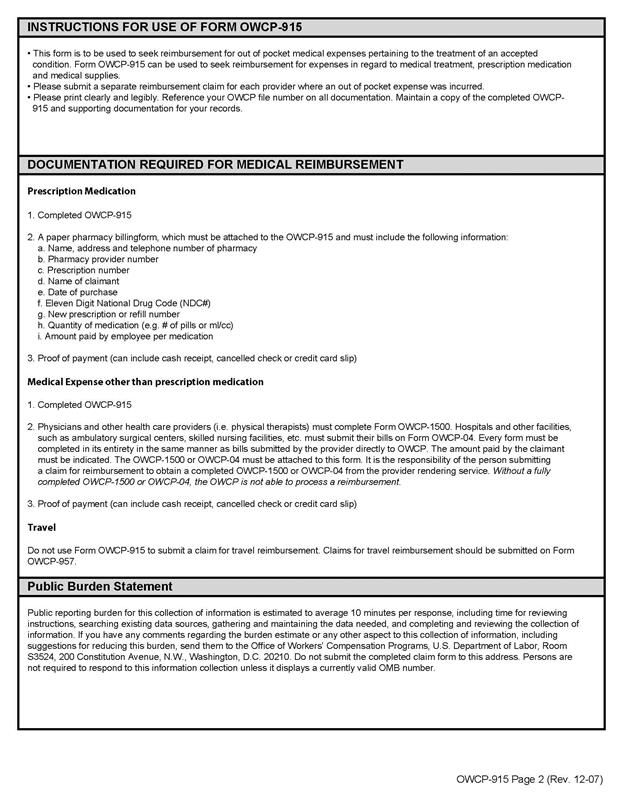
For reimbursement of out-of-pocket medical expenses associated with treatment of your accepted condition, you will need to complete form OWCP-915 Claim for Medical Reimbursement. Use form OWCP-957 Medical Travel Refund Request for obtaining reimbursement of travel costs associated with care for your accepted condition. DEEOIC will only reimburse travel costs directly to you, including any authorized costs associated with a travel companion. I have attached both forms for your convenience. Each form includes instructions for completion and identifies additional documentation required for reimbursement, if applicable.
Please mail your completed forms to:
U.S. Department of Labor
Energy Employees Occupational Illness Compensation Program
P.O. Box 8304
London, KY 40742-8304
In order for providers to bill DEEOIC directly, they must enroll with our bill processing agent (BPA). For questions and information about enrollment and billing, providers should contact our BPA at: 1-844-493-1966. Our agent can explain the Program to your provider(s) and supply them with the necessary forms required for submitting bills for reimbursement. Billing information is also available at the following OWCP website address: https://owcpmed.dol.gov.
If you have questions about the submission or payment of bills, or require any other medical bill program assistance, contact a representative with our BPA, toll free, at 1-866-272-2682.
Sincerely,
Hearing Representative
Enclosures:
Notice Regarding Home and Residential Health Care
Form EE-17A
OWCP-915
OWCP-957
Note: if the DEEOIC pays less than the billed amount (in accordance with the fee schedule), you are not responsible for payment of the difference to a provider. Providers and claimants may submit requests for reconsideration of fee determinations in writing, with accompanying documentation, to the address supplied in this letter.
Division of Energy Employees Occupational Illness Compensation (DEEOIC)
NOTICE REGARDING HOME AND RESIDENTIAL HEALTH CARE
As a beneficiary under the Energy Employees Occupational Illness Compensation Program Act (EEOICPA), you are eligible for many medical benefits, including Home and Residential Health Care. It is important that you receive accurate information about your medical benefits, so we are providing you with important information about how to obtain Home and Residential Health Care (HRHC).
• Authorization for HRHC allows for reimbursement of those medical costs linked to caring for your accepted work-related illness. You do not have to apply for HRHC authorization until you and your physician agree that you require in-home care.
• You, or your authorized representative, can initiate a request for HRHC, at any time, by completing, signing, and returning the attached Form EE-17A. Mail your completed form to:
DOL DEEOIC Central Mail Room
PO Box 830
London, KY 40742-8306
You can also fax your form to your district office, your nearest Resource Center, or upload the form to the DEEOIC EDP portal at - www.dol.gov/owcp/energy/regs/compliance/claimant_medprovider_resources/claimant_edp.htm
• Upon receipt of your EE-17A, DEEOIC will contact your designated physician to request the medical information the program needs to authorize your claim for HRHC.
• DEEOIC neither endorses nor sponsors any home health care provider, or any other entity providing medical services. You are free to choose any licensed provider of home health care services, as long as that provider completes the DEEOIC enrollment process. Moreover, you are free to change home health care providers at any time.
DEEOIC will ask your physician to specify the level of care you require to tend to your accepted illness (skilled nursing care, home health aide, etc.); the frequency and the duration of the care required (i.e., number of hours per day or week for each type of care); and the period for which you will require in-home care. To respond, your physician must conduct a face-to-face (in person) assessment of your HRHC needs within 60 days of the submission of medical evidence used to support a request for HRHC.
In conducting a review of HRHC requests, DEEOIC may seek clarifying information from your designated physician. It may also seek the input of nurse consultants or independent medical examiners in assessing the medical necessity of a request for HRHC.
If you have questions about the HRHC authorization process, contact your district office Claims Examiner or your assigned Medical Benefits Examiner.